Myofascial pain syndrome is a chronic condition characterized by sensitive trigger points within muscle tissue that cause localized or referred pain. These areas of taut muscle fibers restrict range of motion and often persist despite standard rest.
Physical therapy serves as the primary intervention to normalize muscle tone and restore function. By targeting these specific tension centers, therapists interrupt the cycle of chronic discomfort and prevent the development of compensatory movement patterns.
This guide details the role of clinical physical therapy in managing myofascial pain, explores evidence-based release techniques and modalities, outlines recovery expectations, provides strategies for effective at-home maintenance, and explains the importance of integrated care in long-term rehabilitation.
Understanding the Role of Physical Therapy in Myofascial Pain Management
Physical therapy for myofascial pain syndrome is a specialized approach focused on identifying and releasing trigger points to restore muscle function.
At PremierMD, our philosophy for myofascial pain syndrome physical therapy treatment centers on breaking the cycle of chronic tension and neurological sensitivity. Rather than merely treating symptoms, physical therapy aims to restore the mechanical integrity of the musculoskeletal system by lengthening shortened tissues and improving blood flow to oxygen-deprived “knots.” According to experts at the Mayo Clinic, a comprehensive treatment plan often integrates physical therapy with other modalities, such as trigger point injections, to effectively manage persistent myofascial discomfort.
Acute Muscle Knots vs. Chronic Myofascial Pain Syndrome
It is important to distinguish between a simple, temporary muscle knot and the complex nature of Myofascial Pain Syndrome (MPS). While anyone can develop a tight muscle after a long day at a desk or a strenuous workout, MPS involves “active” trigger points that persist over time and often cause pain in areas seemingly unrelated to the knot itself. During a physical therapy evaluation, your clinician will look for specific clinical indicators through physical palpation:
- Taut bands: Feeling a rope-like, palpable cord within the muscle fibers that indicates localized tension.
- Local twitch responses: An involuntary contraction or “jump” of the muscle when the trigger point is manually stimulated.
- Referred pain: Pain that radiates or “refers” to a different part of the body when pressure is applied to the specific knot.
- Persistent tenderness: A “spot” within the muscle that is exquisitely sensitive to even light pressure.
By identifying these specific markers, physical therapists can determine which muscles are the primary drivers of your dysfunction. This diagnostic process is the first step toward applying targeted, evidence-based interventions to provide lasting relief.
Evidence-Based Techniques and Modalities for Trigger Point Release
Successfully managing myofascial pain syndrome physical therapy treatment requires a combination of skilled manual intervention and supportive clinical modalities. Because myofascial trigger points involve both physical knots in the muscle and sensitized nerve endings, a multifaceted approach is necessary to “reset” the affected tissue. Clinical evidence emphasizes that while home stretching is helpful, professional intervention often provides the catalyst for significant recovery.
Manual Release vs. Dry Needling: Which is More Effective?
Research consistently indicates that both manual trigger point release and dry needling are highly effective, though they offer different clinical advantages. Studies suggest that dry needling may provide faster short-term pain reduction and immediate improvements in range of motion by directly eliciting a local twitch response. Conversely, manual release (ischemic compression) is often cited for its superior long-term outcomes in patient comfort and its ability to address the surrounding connective tissue without the invasive nature of needles.
In many cases, the most effective protocol is a hybrid approach. For example, a patient might receive trigger point injections or acupuncture to desensitize a highly reactive knot, followed by manual myofascial release to restore elasticity to the muscle fibers.
Supplemental Modalities for Enhanced Recovery
Beyond direct pressure or needling, several supplemental modalities are used to facilitate healing and reduce the discomfort associated with treatment:
- Therapeutic Ultrasound: Uses high-frequency sound waves to generate deep heat within the muscle, improving local circulation and making the trigger point more pliable for manual release.
- Electrical Stimulation (E-Stim): Delivers low-voltage currents to the muscle to disrupt pain signals and fatigue hyperactive muscle fibers into a state of relaxation.
- Thermal Therapy: The strategic application of heat to increase blood flow or cold to reduce post-treatment inflammation is a staple of a professional American Physical Therapy Association (APTA) recommended care plan.
Checklist: How to Verify Your Therapist’s Myofascial Training
Not all physical therapy focuses on myofascial release. To ensure you are receiving specialized care for myofascial pain syndrome, use the following checklist when selecting a provider or verifying their credentials:
- [ ] Does the provider hold a Certified Myofascial Trigger Point Therapist (CMTPT) credential?
- [ ] Is the clinician trained in manual therapy through recognized organizations like the APTA or similar accredited bodies?
- [ ] Does the clinic offer a combined approach, including both passive modalities (ultrasound, heat) and active therapies (corrective exercise)?
- [ ] Is there a clear emphasis on functional assessment to determine why the trigger points formed in the first place?
- [ ] Does the therapist have specific experience in dry needling or working alongside physicians for integrated care?
Choosing a provider with these specific qualifications ensures that your treatment targets the root cause of your muscle dysfunction rather than just masking the symptoms. By integrating these advanced modalities, patients can transition from acute pain management to long-term postural and muscular health.
What to Expect: Pain Levels, Session Frequency, and Relief Timelines
Understanding ‘Good Pain’ During Trigger Point Release
A trigger point release typically feels like a deep, “productive” ache that mimics the referred pain pattern of the muscle being treated. While the pressure may be intense, it should feel like a releasing sensation—often described by patients as “good pain”—rather than a sharp or radiating electrical sting.
Following a session of myofascial pain syndrome physical therapy treatment, it is common to experience localized soreness similar to the feeling after a strenuous workout. This sensitivity usually peaks within 24 hours and subsides by the second or third day as the muscle tissue begins to remodel and local circulation improves.
Standard Recovery Timeline
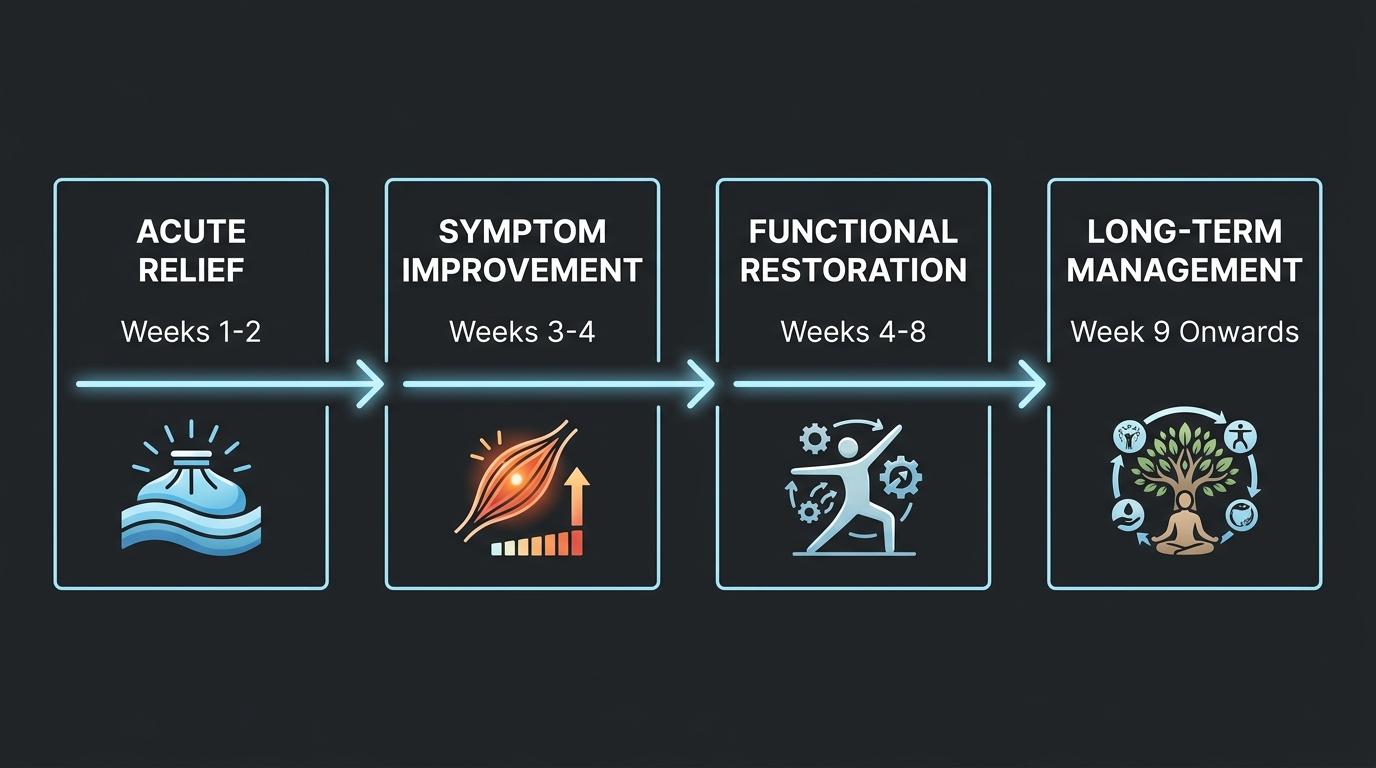
Recovery from chronic myofascial pain is a cumulative process. While some patients feel immediate relief after a single session, lasting functional changes require consistent intervention to “retrain” the nervous system and muscle fibers.
| Phase | Focus | Frequency | Typical Duration |
| Acute Relief | Reducing immediate pain and deactivating hyper-irritable spots. | 2–3 sessions per week | 1–2 weeks |
| Sub-acute | Improving tissue mobility and restoring range of motion. | 1–2 sessions per week | 2–4 weeks |
| Functional Restoration | Strengthening and postural correction to prevent recurrence. | Once a week or bi-weekly | 4–8+ weeks |
Managing Temporary Symptom Flare-Ups
It is not uncommon for symptoms to temporarily fluctuate during the first few weeks of treatment. As deep-seated muscle tension is released, your body may react with a brief “flare-up” as it adjusts to new alignment and improved blood flow. These episodes are generally shorter and less intense than the original pain and serve as a sign that the neuromuscular system is responding to the therapy.
To support the recovery process between visits to PremierMD, your provider will transition you toward at-home care strategies. This ensures that the progress made during trigger point injections or manual therapy is maintained through daily activity.
At-Home Care: Self-Massage, Stretching, and Lifestyle Habits
Managing myofascial pain syndrome requires a proactive approach between office visits. While professional physical therapy treatment provides the foundation, daily maintenance through self-massage and ergonomic awareness prevents “knots” from returning and maintains muscle elasticity.
How to Use Foam Rollers and Self-Massage Tools
Foam rollers, lacrosse balls, and massage canes are effective for “autonomy-based” trigger point release. Follow these steps to ensure you are treating the tissue without causing unnecessary inflammation:
- Identify the trigger point: Gently palpate the muscle to find the specific “knot” or area of peak sensitivity that may radiate pain elsewhere.
- Position the tool: Place the foam roller or massage ball directly under the target muscle, using your body weight to apply moderate pressure.
- Roll slowly: Move the tool at a rate of about one inch per second. Avoid rolling directly over bony prominences or joints.
- Pin and hold: When you hit a particularly tender spot, stop rolling. Maintain steady pressure for 30 to 60 seconds until you feel the muscle “melt” or the intensity of the pain decrease.
- Breathe deeply: Use diaphragmatic breathing to signal your nervous system to relax, which aids in the release of the fascia.
Daily Stretches for Myofascial Relief
Consistency is more important than intensity when stretching for myofascial pain. Use these movements to keep the fascia hydrated and pliable:
- To release neck and upper trap tension: Perform Chin Tucks by pulling your head straight back (creating a “double chin”) to realign the cervical spine and decompress the suboccipital muscles.
- To alleviate chest tightness and rounded shoulders: Use the Doorway Stretch, placing your forearms on either side of a door frame and leaning forward to open the pectoral muscles.
- To reduce lower back and glute pain: Practice the Pigeon Pose or a seated figure-four stretch to elongate the piriformis and deep hip rotators.
- To improve mid-back mobility: Engage in Cat-Cow movements to gently mobilize the fascia surrounding the thoracic spine.
Lifestyle Adjustments for Long-Term Management
Small shifts in your daily routine can significantly reduce the frequency of myofascial flare-ups:
- Prioritize Hydration: Fascia is primarily composed of water. Dehydrated tissue becomes sticky and prone to adhesions, so aim for consistent fluid intake throughout the day.
- Optimize Ergonomics: Ensure your computer monitor is at eye level and your chair provides adequate lumbar support to prevent “text neck” and postural strain.
- Manage Stress: Since myofascial pain is often exacerbated by subconscious muscle clenching, integrating mindfulness or medical acupuncture can help lower systemic tension.
- Movement Breaks: Follow the 20/20 rule—every 20 minutes, stand up and move for at least 20 seconds to prevent the fascia from “setting” in a shortened position.
While these at-home strategies are vital, stubborn trigger points may require clinical intervention. If self-care does not provide adequate relief, trigger point injections or specialized cupping therapy can help reset the muscle tissue, making your at-home stretching much more effective.
The Synergy Between Family Medicine and Myofascial Recovery
Primary care providers serve as the essential first line of defense for patients navigating the complexities of chronic musculoskeletal pain. One of the most critical diagnostic challenges in family medicine is accurately distinguishing between Myofascial Pain Syndrome (MPS) and Fibromyalgia. While these conditions often overlap in clinical presentation, their underlying mechanisms require different therapeutic paths. A primary care physician trained in integrated medicine can identify whether a patient’s pain is regional and tied to specific trigger points or if it is part of a systemic, widespread condition. Identifying this distinction early is vital for implementing the correct myofascial pain syndrome physical therapy treatment and avoiding unnecessary or ineffective interventions.
| Feature | Myofascial Pain Syndrome (MPS) | Fibromyalgia |
| Pain Distribution | Regional or localized to specific muscle groups. | Widespread; typically affects all four quadrants of the body. |
| Physical Findings | Presence of taut muscle bands and focal trigger points. | Generalized tender points and systemic sensitivity. |
| Pain Referral | Pressure on a point causes pain in a predictable, distant area. | Pressure causes localized pain without a specific referral pattern. |
| Associated Symptoms | Localized weakness and restricted range of motion. | Chronic fatigue, sleep disturbances, and “fibro fog.” |
| Primary Treatment | Physical therapy, myofascial release, and Trigger Point Injections. | Multidisciplinary care focusing on central nervous system regulation. |
Integrating Eastern and Western Medicine
At PremierMD, we believe the most effective recovery plans bridge the gap between traditional Western interventions and evidence-based Eastern modalities. By combining physical therapy and medical procedures like Trigger Point Injections with medical acupuncture, we address pain from both a mechanical and systemic perspective.
While Western techniques are exceptional at deactivating the physical “knot” within the muscle, Eastern practices such as acupuncture and cupping help to modulate the nervous system, improve local circulation, and reduce the inflammatory markers that contribute to chronic tension. This integrated approach ensures that we are not simply treating a symptom, but are instead optimizing the body’s environment for long-term myofascial healing.
A comprehensive pain management strategy is most successful when it is overseen by a primary care team that understands the full spectrum of your health. By leveraging the synergy between specialized physical modalities and holistic wellness, patients can move beyond temporary relief toward a sustainable, pain-free lifestyle.
Frequently Asked Questions About Myofascial Physical Therapy
Can I use heat or ice for myofascial pain?
Heat is generally the most effective choice for myofascial pain because it helps relax tight muscle fibers and increases blood flow to the restricted trigger point area. While ice may be used to reduce acute inflammation immediately after an injury, moist heat is preferred for chronic myofascial pain syndrome physical therapy treatment as it helps “soften” the fascia and eases muscle tension. Applying heat for 15–20 minutes before performing your prescribed stretches can significantly improve mobility.
Is myofascial pain syndrome permanent?
No, myofascial pain syndrome is not permanent and can be successfully resolved or managed through targeted physical therapy and lifestyle modifications. While the condition can become chronic if the underlying movement patterns are not addressed, most patients experience significant relief once they begin a structured program of manual therapy, trigger point injections, and corrective exercise. Consistency is the key to preventing the recurrence of active trigger points.
How does stress contribute to trigger points?
Stress is a primary trigger for myofascial knots because it causes the body to remain in a state of constant physical “bracing” or muscle tension, particularly in the neck, shoulders, and jaw. This chronic contraction restricts oxygen and blood flow to the muscle tissue, creating the perfect environment for trigger points to form. Furthermore, emotional stress increases the nervous system’s sensitivity to pain, making existing knots feel more severe. Integrated approaches, such as acupuncture for pain management, are often effective in addressing the neurological component of stress-related pain.
Can myofascial pain cause headaches or tingling?
Yes, myofascial pain syndrome frequently causes headaches and tingling sensations through a process called referred pain. Trigger points in the trapezius or cervical muscles are a leading cause of tension-type headaches, as the pain radiates from the “knot” up into the skull. Additionally, if a tight band of muscle or inflamed fascia compresses a nearby nerve, it can cause paresthesia, which manifests as tingling or “pins and needles” in your arms or legs.
[insert diagram of common referred pain patterns for tension headaches here]
Frequently Asked Questions About Myofascial Pain
Can I use heat or ice for myofascial pain at home?
Both heat and ice serve specific purposes in managing muscle tension. Applying heat is generally preferred for chronic stiffness because it increases blood flow and helps relax the taut bands associated with trigger points. Ice is most effective for numbing acute pain or reducing localized soreness that might occur after an intense physical therapy session. Many patients find the greatest relief by using heat before performing their prescribed stretches to make the tissue more pliable.
Is myofascial pain syndrome permanent?
This condition is not permanent for those who engage in active treatment and lifestyle modification. While the pain can feel persistent if the root causes are left unaddressed, physical therapy and specialized medical interventions are highly effective at breaking the pain-spasm cycle. Most individuals experience significant functional recovery once they identify and correct the underlying postural or repetitive strain issues that sustain the trigger points.
How does stress contribute to myofascial trigger points?
Stress acts as a primary catalyst for muscle tension by triggering the body’s involuntary guarding response. When you are under pressure, your muscles remain in a constant state of low-level contraction, which deprives the tissue of oxygen and promotes the formation of painful knots. Managing mental well-being is often just as critical as physical exercise in preventing the recurrence of chronic myofascial symptoms.
Can myofascial pain cause referred symptoms like headaches or tingling?
Referred pain is a hallmark of this syndrome, where a trigger point in one muscle sends pain signals to a completely different part of the body. For example, knots in the upper trapezius or neck muscles are common culprits for tension headaches, while trigger points in the hips can cause tingling sensations that mimic nerve compression in the legs. Resolving these complex symptoms requires a comprehensive approach that looks beyond the immediate area of discomfort to find the true source of the problem.
Start Your Path to Pain-Free Living
Reaching your recovery goals requires a coordinated strategy that bridges the gap between different therapeutic methods. Schedule a consultation with our integrated family medicine team to develop a personalized pain management plan that combines physical therapy, trigger point injections, and acupuncture. Our clinical staff works together to ensure every aspect of your care is aligned for the best possible outcome.
Leave a Reply